Tennis elbow is an overuse condition giving pain in the forearm muscles near the elbow when holding or gripping objects. It is the most common overuse syndrome.
Tennis elbow has been given many names: lateral epicondylitis; lateral epicondyle tendinopathy; lateral elbow tendinopathy; lateral epicondylalgia and more. Lateral epicondyle tendinopathy (LET) is now the official medical name although it’s still referred to as tennis elbow as it’s so easy and familiar.
Lateral epicondyle tendinopathy means an “-opathy” or structural change for the worse, going on in the tendon(s) on the outside of the elbow at the bony protrusion called the epicondyle. Medial epicondyle tendinopathy (golfer’s elbow) is the same condition but occurs on the inside of the elbow.
Tennis elbow is often called an acute tendonitis, but if it has been present for a while there is no evidence of inflammation so we need to give it the different name of tendinopathy to be more accurate.
Tennis Elbow Symptoms
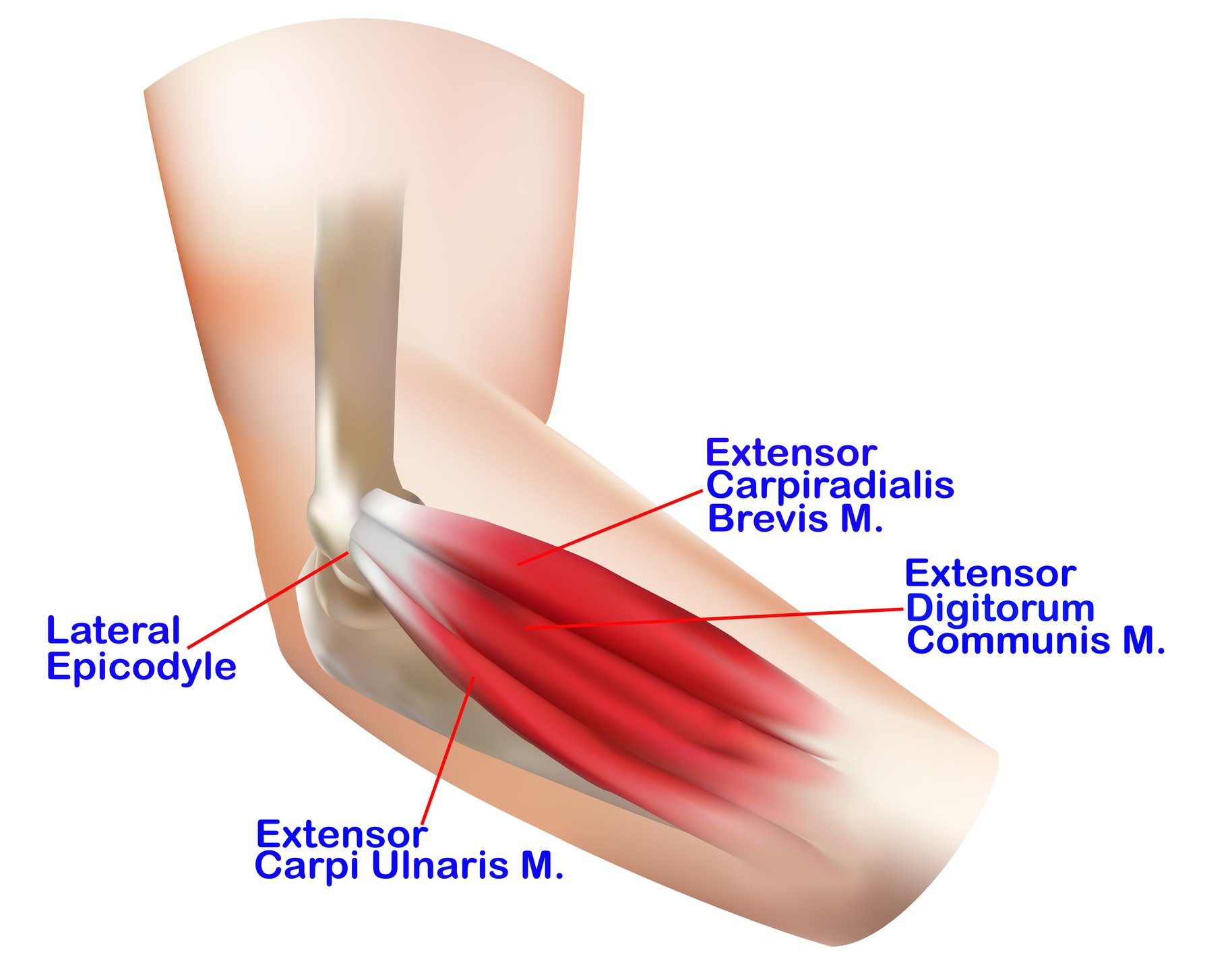
Tennis elbow gives elbow pain where the forearm extensor muscles originate at the lateral epicondyle, brought on by gripping and repetitive manual work. Pain may radiate down the forearm or be present in the shoulder and upper arm.
Who Gets Tennis Elbow?
Tennis (and golfer’s) elbow are commonest in men and women over 40 years of age, with no particular difference between the sexes. It’s most prevalent between 35 and 55 years of age and at any one time is occurring in about 1-3% of the population.
By our forties our tendons have changed since our twenties, though they work perfectly well most of the time. However overdoing things can inflame a tendon, cause changes within its structure or in extreme cases cause it to rupture, although this last event is uncommon.
Tennis Elbow Pathology
Tendons “insert” into our bones, anchoring to the bone so the muscle can pull as required. Just before they enter the bone there is a zone that is poor in blood supply which increases the possibility of degenerative changes occurring there. This happens most commonly at about 1-2cm from the insertion of the tendon of the extensor carpi radialis brevis muscle.
On surgical operation a normal tendon looks white and shiny and is firm to pressure. A degenerative tendon appears grey, swollen and flaky and is abnormal under microscopic examination.
Under the microscope signs of inflammation are not usually present but there is an increase in the number of blood vessels and fibroblasts (these make collagen which tendons consist of). There are also tears in and disruption of the collagen structure of the tendon.
Risk Factors for Tennis Elbow
While the pathology underlying this condition is not completely clear, it has been connected with some risk factors. These include handling heavy loads frequently and performing repetitive arm and hand movements for some hours a day.
In normal life this means that anything we do with our hands at a higher level than normal in terms of force and repetition can bring on tennis elbow.
Tennis elbow does occur in people who play tennis, but different playing techniques used today have reduced the incidence to a minority of sufferers.
The Prognosis for Tennis Elbow (how it’s going to go)
It had been thought that most episodes settle down if you don’t continue to re-stress the area by doing more of the aggravating activity. However, one study has found that although there was improvement in 90% of cases in a year, full recovery occurred in only 13% at three months from onset and 34% at twelve months.
Tennis Elbow Treatment
The aims of treatment are:
- Pain control and reduction
- Maintainance of range of movement
- Increasing grip strength and endurance
- Improving the normal ability to use the arm
- Preventing further worsening
Physiotherapy is the first line treatment for tennis elbow. Symptoms may be isolated to the edge of the elbow but can also be in the forearm, in both arms, in the upper arm or shoulder. This might indicate involvement of the spine in the pain production.
A physiotherapist can give a full assessment of the neck, shoulder and arm and set out a treatment plan to address the problem.
Rest and avoiding the aggravating actions may be a good starting point for acute tennis elbow, as this tends to reduce the pain to manageable levels or abolish it completely.
Physiotherapy treatments include strapping, a tennis elbow brace, deep transverse frictions, mobilisation techniques to the elbow and radio-ulnar joint, ultrasound, laser treatment, stretches and eccentric strengthening exercises. Wrist splints have been shown to reduce pain symptoms in tennis elbow.
Eccentric exercises are one of the most promising areas of treatment. This means that the muscle exerts its power while it is lengthening rather than shortening. Eccentric exercises usually need to be supervised by a physiotherapist as they are difficult to get exactly right to start with. Once the pain is brought under control the physiotherapist will move on to increasing the muscle power of the grip in functional situations.
Tennis Elbow Surgery
Tennis elbow surgery is an effective treatment for symptoms that don’t respond to other interventions. It involves cutting away the tendon of the ECRB muscle from the bone and in some cases cutting away the bone surface where the tendon attaches. The tendon may be lengthened and repaired so the muscle continues to function.
Surgery can be performed as a traditional, open technique or by using the arthroscope. Both techniques give good to excellent results in 80-90% of patients but arthroscopy may give slightly better outcomes overall.
Alternative Treatments
A large number of treatments have been explored and these include:
• Extracorporeal shock wave therapy (ECSW) directs shock waves at the tendon. The method of action of this treatment is not clearly known and NICE recommends more research into this method to clarify if it is likely to be useful.
• Laser therapy. Mostly applied by physiotherapists, laser energy is thought to stimulate collagen production in the tendon. A short-term benefit has been shown to occur.
• Acupuncture. A short-term benefit is again possible.
• Injections of various substances. Botulinum toxin has not been shown to be useful. Injecting the person’s own blood back into the site (autologous blood injection) may stimulate an inflammatory reaction but the usefulness of this has not yet been determined. Concentrated platelets (platelet rich plasma) are also injected but the same applies as to the blood injection above.
The Grip
Strong gripping involves co-contraction, with the flexor and extensor muscle groups working together at the same time. Without the extensors you can’t get good grip strength just from the flexor muscles.
When you grip you will see your wrist instantly moves up into extension and your knuckles point upwards. This is the power grip position and any other wrist position reduces grip power.
In the power grip the wrist flexors and extensors are not producing grip power as such, they hold the wrist in the best position for gripping and allow the finger flexor muscles to exert the grip power to hold something.
The wrist flexors are 62% stronger than the extensors. This means that the wrist extensors’ ability to hold the wrist position with enough power and endurance will dictate how strongly you can grip and for how long.
Being the smaller and weaker muscle group than the flexors, the extensors may be the limiting factor, weakening early and letting the power position fail. This will then let the grip fail. So it’s important to have strong extensors which can keep up a contraction for as long as you want to maintain your grip. Tennis elbow pain limits the ability of the extensors to do their job and so weakens the grip.
References:
- Associations between work-related factors and specific disorders at the elbow: a systematic literature review. Rogier M. van Rijn and others, Rheumatology, 2009.
- A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia. L Bisset and others, British Journal of Sport Medicine 2005; 39:411-422.
- The management of tennis elbow. J Orchard, A Kountouris, BMJ 2011;342.
- Common overuse tendon problems: A review and recommendations for treatment. JJ Wilson and TM Best, 2005, Bot SDM et al. Annals of Rheumatic Diseases 2005; 64: 1331-1336
- An exercise programme for the management of lateral elbow tendinopathy. D Stasinopoulous, K Stasinopoulous, MI Johnson. British Journal of Sports Medicine, 2005;39:944-947.
- Medscape – Bryant James Walrod, MD Assistant Clinical Professor, Department of Family Medicine – Bot SDM et al. Annals of Rheumatic Diseases 2005; 64: 1331-1336
- Course and prognosis of elbow complaints: A cohort study in general practice. Bot SDM et al. Annals of Rheumatic Diseases 2005; 64: 1331-1336.
- Lateral epicondylitis. A review of pathology and management. Instructional Review: Shoulder and Elbow. Bot SDM et al. Annals of Rheumatic Diseases 2005; 64: 1331-1336
Last Review Date: 01-04-2018
Next Review Date: 01-04-2020
{kind=link}