Rotator cuff tears are tears in the tendons of the muscles that control much of the shoulder’s stability and mobility. This is usually a degenerative process associated with ageing although repetitive use or trauma can cause similar problems in younger people. The saying “Grey hair equals cuff tear”, when an older patient consults a shoulder specialist, indicates which age group this is most common in.
Rotator Cuff Anatomy
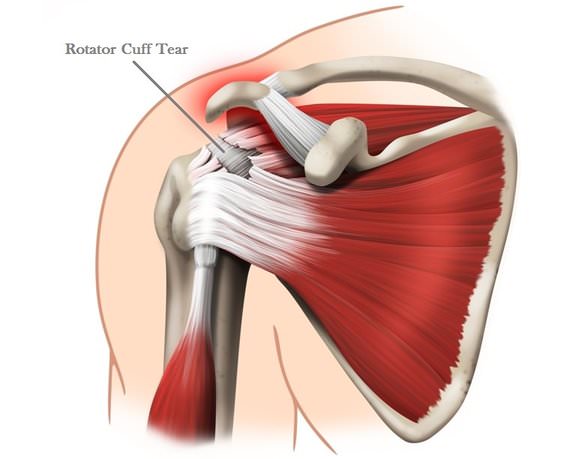
The rotator cuff is a group of four muscles (supraspinatus, infraspinatus, teres minor and subscapularis) that originate on the shoulder blade or scapula.
These muscles all lead towards the head of the humerus, gradually becoming more fibrous until they merge into a sheet of fibrous tissue and insert into the bone. This cuff of four muscles surrounds the head of the humerus, stabilises the shoulder and allows the powerful deltoid muscle to move the arm.
Who Gets A Rotator Cuff Tear?
There are two main groups:
- Younger people who either have some trauma like a fall from a bike or have been doing a lot of overhead activities. In these patients, the rotator cuff is normal until it is severely stressed.
- Older people have a gradual onset of shoulder pain and later may show tears on MRI scanning but have no history of trauma. Rotator cuff tears are common in people over 60 but many give no symptoms. Around 40% of people over 60 years old were found to have full-thickness tears in a study on cadavers. The frequency of rotator cuff problems rises with age.
Rotator Cuff Symptoms
- Shoulder pain over the front of the shoulder and is worse doing overhead activities. The shoulder may often be painful at night, particularly when lying on that side.
- Weakness of the shoulder will be related to lack of use and the degree of pain present.
- Loss of active shoulder motion may be observed. Patients may be unable to lift their own arm up fully but an examiner can do it for them.
Causes of Rotator Cuff Tears
- Degenerative changes within the tendons. This is an age-related process and referred to as tendinopathy. Achilles tendinopathy is another example.
- Poor blood supply to parts of the tendons, giving them less ability to maintain themselves when stressed and less ability to heal after an injury.
- The bony shape of part of the shoulder region above the rotator cuff (the acromion) has been shown to vary may be important in cuff tears. This may be a secondary effect (i.e. not the cause) due to weakness allowing the head of the humerus to impinge under the acromion and cause the bony changes.
- Weakness of the rotator cuff muscles can increase the stresses on the static parts of the joint and allow the head of the humerus to move abnormally.
- Impingement. This occurs when the top of the head of the humerus causes pressure against the underside of the acromion above. The supraspinatus tendon is in this area and is thought to suffer tendinitis and tears in more severe cases.
- Instability. Laxity of the ligaments may be inherited or due to stretching for athletic performance. This allows the head of the humerus to move upwards and impinge on the structures above, eventually injuring the rotator cuff.
Rotator Cuff Tear Treatment
In the acute phase, physiotherapy is aimed at reducing pain and inflammation in the shoulder. Ice, rest from aggravating activities, change in sleeping position and painkillers are the main approaches. Corticosteroid injection into the shoulder joint may be considered.
Physiotherapy for Rotator Cuff Pain
- Restoration of full movement to the shoulder. The movement of the shoulder joint and the scapula occurs in a particular pattern and that needs to be restored if it has been affected.
- Strengthening the muscles of the shoulder blade and shoulder. Muscles that need to be strengthened may include the trunk muscles which stabilise the shoulder blade, the rotator cuff muscles themselves and the large shoulder muscle (deltoid).
- Restoration of the joint position sense (JPS or proprioception). This allows the joint to be in the right position at all times during activities and is essential for the balanced production of strength by the shoulder.
- Training in sport or task-specific activities.
Surgery For Rotator Cuff Tears – Rotator Cuff Repair
If pain and function do not improve after a few months of physiotherapy then a surgical approach may be tried in active individuals. Tears may be stitched if the gap is not too great and part of the acromion may be removed if it is thought to be a contributing factor. Early repair (within three weeks) is indicated after a sudden injury as this may prevent the cuff muscles from degenerating.
Large muscle tears may not be operable but in some cases tendon transfers may help reduce pain and improve movement.
Post-operative care for rotator cuff repair is very specific and the physiotherapist will follow the surgeon’s protocol. The timing of increased stresses to be put through the repair is critical. Patients often report significant pain in the few weeks after operation and rehabilitation can take six months to a year to get to the best result. Physiotherapy may need to be continued for three months or longer.
References:
- Rotator Cuff Tear. OrthoInfo. American Academy of Orthopaedic Surgeons AAOS. http://orthoinfo.aaos.org/topic.cfm?topic=A00064?
- Rotator Cuff Arthropathy: Evaluation, Diagnosis and Treatment. Nam D et al. Journal of Bone and Joint Surgery Am March 2012, 94(6) (abstract).
Last Review Date: 25-02-2020
Next Review Date: 25-02-2022
{kind=link}