Neck strains and sprains are among the most common musculoskeletal injuries. In cases where neck pain results from rapid acceleration and deceleration, such as during a car crash or sporting injury, it is often referred to as Whiplash Syndrome or Whiplash Associated Disorder (WAD).
Neck Anatomy
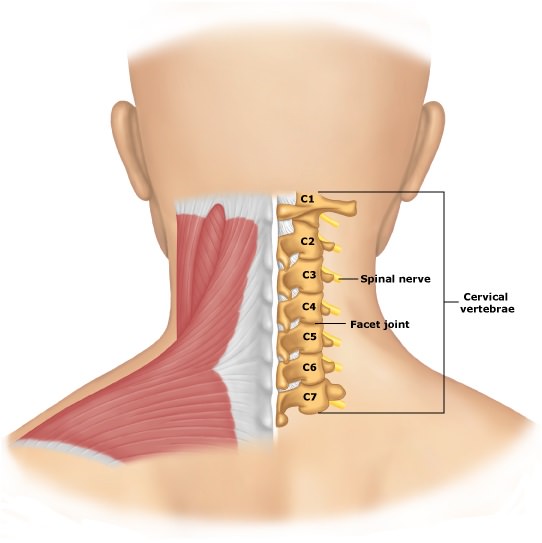
The neck is composed of seven cervical vertebrae stacked on top of one another, separated by intervertebral discs. The top two vertebrae are uniquely designed for head rotation and flexion/extension (bending forwards and backwards).
As the head is heavy and is sits atop the slender neck, sudden forces can easily strain the neck, magnifying the stress on the cervical vertebrae.
Who Gets A Cervical Strain Or Whiplash?
Chronic neck strains account for nearly 85% of neck pain cases. These neck strains are often caused by repetitive activities such as lifting, pulling, awkward sleep posture or sitting in poor positions for extended periods, such as while using a computer.
Additionally, whiplash injuries are common, especially in rear-end car collisions, affecting approximately 1 in 1,000 people annually. Whiplash Syndrome not only leads to persistent neck pain but also significantly impacts disability rates and healthcare costs.
Cervical Sprain And Whiplash Symptoms
Symptoms of cervical sprain or whiplash can occur immediately or within 12 to 72 hours after an incident. Common symptoms include:
- Neck pain
- Occipital headache (pain at the back of the neck)
- Muscle spasms
- Pain in the upper back, shoulders or arms
- Dizziness and tinnitus
- Weakness in the arms, memory problems, altered concentration and sleep disturbances
Effective Treatment for Cervical Sprain and Whiplash
Early rehabilitation is crucial to prevent long-term pain and disability. Physiotherapy plays a key role in recovery, with passive treatments used initially, followed by active treatments as soon as possible. Passive treatments include ice, heat, massage, neck traction and joint mobilisation. While active treatments focus on neck exercises, stretches and fitness work.
The goal of physiotherapy is to restore neck and upper body function, reducing the risk of chronic issues and encouraging a return to daily activities, including work. It is important to return to work even if some pain persists, as early return has been associated with better outcomes.
Strengthening deep postural muscles in the neck has proven effective in improving functionality. Active physiotherapy has also been shown to be more cost-effective than other treatment methods. In chronic cases of whiplash or neck sprain, manual therapy and manipulation have been shown to provide relief.
Surgery is rarely required unless there is spinal cord or nerve root compression. For persistent pain, radiofrequency neurotomy can block pain transmission from facet joints by damaging the nerves responsible. Other options for managing chronic pain include pain management programs, botulinum toxin injections and steroid injections.
References:
- Neck pain and stiff neck. NHS Choices. http://www.nhs.uk/conditions/Neck-pain/Pages/Introduction.aspx
- Neck pain – whiplash injury. NICE. http://cks.nice.org.uk/neck-pain-whiplash-injury#!topicsummary
Last Review Date: 20-10-2024
Next Review Date: 19-10-2025
{kind=link}